Remote patient monitoring adoption hindered by systemic policy gaps
Despite advancements in wearable health technology, systemic policy barriers continue to prevent remote patient monitoring from moving beyond pilot programs.
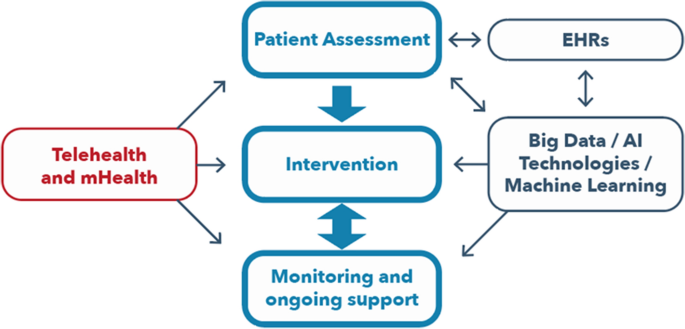
Remote patient monitoring (RPM) represents a significant shift in the delivery of modern healthcare, offering the potential to extend clinical oversight beyond hospital walls. By utilizing wearable sensors, connected blood-pressure cuffs, smart scales, and smartphone-based mobile health (mHealth) applications, providers can collect continuous data to manage chronic conditions. Despite this technical maturity, the integration of these tools into routine, sustainable medical practice remains hindered by systemic policy gaps that prevent RPM from scaling beyond temporary pilots or emergency-era mandates.
The reliance on short-term programs was highlighted by the COVID-19 pandemic. During global lockdowns, regulatory and reimbursement barriers were temporarily relaxed, allowing telemonitoring and virtual care to expand rapidly. However, once emergency rules expired, many of these initiatives contracted or weakened. According to analysis published by Devdiscourse, this pattern suggests that the primary constraint is not the capability of the technology, but rather the absence of permanent, sustainable infrastructure to govern, finance, and support remote care.
Structural Barriers to Adoption
The current landscape of remote care faces four primary systemic challenges that must be addressed to move beyond "pocketed" implementation:
- Provider Economics: Most health payment models remain anchored to episodic, volume-based encounters rather than the asynchronous, continuous work generated by remote data streams. Providers currently lack reimbursement mechanisms for the labor-intensive tasks inherent in RPM, such as alert management, clinical review, patient outreach, and care coordination. Without financial sustainability, these programs often depend on grants, philanthropy, or overextended staff.
- Professional Liability: Continuous observation raises unresolved legal questions regarding the standard of care. There is a lack of clear frameworks defining the required response speed for incoming data alerts or the division of responsibility between device manufacturers, software vendors, AI developers, and clinical teams. Clinicians are often reluctant to assume unlimited responsibility for data streams they are not staffed to monitor.
- Privacy and Equity: Patients frequently encounter opaque data-sharing practices and complex consent forms that may not support meaningful understanding of how their information is used. Furthermore, concerns regarding digital exclusion persist; rural and low-resource settings may face barriers due to limited access to high-speed internet or the technical literacy required to navigate complex health applications.
- Engagement and Adherence: RPM success depends on patient retention, yet many programs struggle with attrition. Experts argue that engagement — tracked through enrollment rates, data-transmission completeness, and alert response — must be treated as a primary outcome measure rather than a secondary concern to avoid widening disparities between those who can participate in digital care and those who cannot.
Digital Health in Specialized Care
The challenges of system-wide integration are particularly visible in obesity management, a multifactorial condition where digital tools are increasingly utilized to bridge the gap between periodic in-person visits. Research published in the journal Clinical Medicine indicates that while these tools facilitate engagement, evidence for their long-term effectiveness remains limited. Most studies focus on short-term results, and there is a documented lack of data regarding the comparative effectiveness of mHealth interventions across different socioeconomic and ethnic groups. Consequently, clinicians are encouraged to direct patients toward clinically proven products, such as those listed in the Organisation for the Review of Care and Health Apps (ORCHA) library, rather than commercially available apps, the vast majority of which are not supported by clinical studies.
The Path Toward Sustainability
As health systems look to modernize, the role of Electronic Health Records (EHRs) has become central to longitudinal oversight. EHRs are being used to improve the coordination of patient care and to assess national performance. For example, the United Kingdom’s National Obesity Audit (2021–2024) leverages routinely collected data to assess adherence to national guidance and track long-term health outcomes. By integrating these datasets, researchers hope to better understand the long-term impact of prescribed digital therapeutics.
The consensus among researchers is that the future of remote monitoring relies on three foundational developments: the formalization of reimbursement models that reward care coordination over volume-based visits; the establishment of legal frameworks to clarify liability in AI-assisted triage environments; and a commitment to digital inclusion that ensures tools are accessible to vulnerable populations. Until policy makers align the rules of the healthcare system with the capabilities of modern monitoring technology, the sector will likely continue to face a paradox: high clinical potential contrasted with significant challenges in routine, sustainable implementation.


