Steatotic liver disease diagnosis requires longitudinal reassessment
Researchers argue that steatotic liver disease should be managed as an evolving trajectory rather than a static diagnosis to account for fluctuating metabolic and alcohol-related risks.
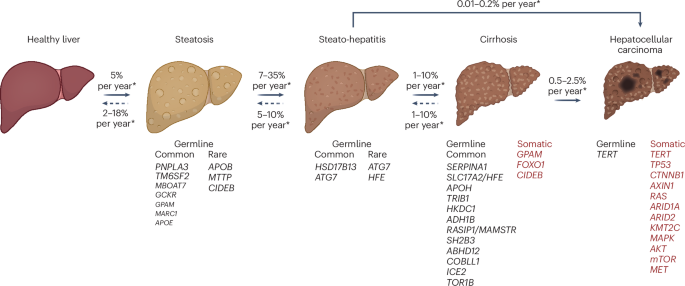
Steatotic liver disease (SLD) comprises a spectrum of conditions, including metabolic dysfunction-associated steatotic liver disease (MASLD), metabolic dysfunction and alcohol-associated liver disease (MetALD), and alcohol-associated liver disease (ALD). Researchers from Charité - Universitätsmedizin Berlin argue that these categories should be viewed as interconnected, evolving disease trajectories rather than rigid, isolated diagnoses. This shift in perspective reflects the biological reality that metabolic health and alcohol intake are highly dynamic, leading to frequent transitions between these sub-classifications.
The argument for a new framework is supported by evidence of clinical instability. In prospective cohort data tracked over a 6-month period, 36% of individuals initially diagnosed with MetALD transitioned into either MASLD or ALD. Similar volatility appeared in the ALD group, where 32% of patients shifted to other subclasses. Even MASLD, the group found to be most stable, saw 11% of patients reclassified within the same period. These shifts occur because alcohol exposure and metabolic dysfunction, such as obesity, type 2 diabetes, dyslipidemia, and hypertension, fluctuate over time and interact in a reciprocal manner. Alcohol can exacerbate metabolic risk factors, while metabolic dysfunction can increase the liver’s vulnerability to alcohol-related damage.
Media additions

Challenges in Diagnostic Accuracy
A central obstacle to a stable classification system is the difficulty of measuring alcohol intake. Current clinical practice relies heavily on self-reported data, which can under-report actual consumption by as much as 57.7%. Because the boundaries between MASLD and MetALD often hinge on specific alcohol thresholds, this reliance on patient history can lead to persistent misclassification and delayed intervention. The authors note that while cumulative lifetime alcohol exposure is clinically significant, there are no universally standardized thresholds for it, and the impact of alcohol is further modified by a patient's age, sex, and metabolic status.
To move toward more objective diagnosis, experts advocate for the use of blood-based biomarkers such as phosphatidylethanol (PEth). Unlike subjective questionnaires, PEth reflects alcohol consumption over the preceding 1–3 weeks and is less influenced by factors like body mass index or biological sex. According to expert guidance, concentrations below 20 ng/mL generally exclude clinically relevant alcohol consumption; levels between 20–200 ng/mL are consistent with MetALD; and levels at or above 200 ng/mL suggest harmful drinking. Other tools, such as ethyl glucuronide (EtG) in hair or urine, can further assist in assessing recent or harmful intake. However, clinicians are advised that these biomarkers should supplement, not replace, clinical judgment and careful history-taking.
Reframing Management
Because simple hepatic steatosis is not always associated with mortality, the authors emphasize that long-term health outcomes in SLD are driven primarily by the progression of liver fibrosis. Therefore, management should prioritize non-invasive assessments, specifically the fibrosis-4 (FIB-4) index and vibration-controlled transient elastography (VCTE), to determine care intensity. Risk-stratification follows a tiered system: low risk (FIB-4 <1.3), moderate risk (FIB-4 of 1.3–2.67 plus VCTE <8 kPa), and high risk (FIB-4 >2.67 or FIB-4 of 1.3–2.67 plus VCTE ≥8 kPa). A higher threshold of FIB-4 >2.0 is used for individuals older than 65 years.
The proposed longitudinal risk-management model would require patients' records to explicitly track three components at every follow-up: the SLD subclass, the stage of fibrosis, and current trajectory markers—including metabolic trends and objective alcohol biomarkers. This approach moves the clinical focus from assigning a static label to managing a dynamic disease process.
Future Implications
This dynamic framework is expected to impact how future clinical trials and treatment protocols are designed. As new therapies, such as GLP-1 receptor agonists and thyroid hormone receptor-β agonists, enter clinical practice, researchers will need to account for the shifting nature of SLD subclasses. Without longitudinal reassessment, the variability in a patient's status could complicate the interpretation of treatment responses. Ongoing and future studies are expected to integrate repeated measures of alcohol exposure and metabolic indicators to establish standardized thresholds for these transitions, helping to align clinical practice with the underlying biology of the disease.


