
Urinary tract infections like cystitis are among the most common bacterial infections worldwide, with women accounting for roughly 80% of cases. Yet a persistent myth—that sitting on public toilet seats spreads the infection—has led many to avoid public restrooms unnecessarily. New public health guidance clarifies what actually increases risk and how to protect yourself during the summer travel season, when exposure to germs rises.
Key Findings
- No direct transmission: Cystitis is not spread by contact with toilet seats, according to infectious disease specialists.
- Primary risk factors: Bacterial entry through the urethra (often from poor hygiene, sexual activity, or holding urine) drives infections.
- Summer-specific risks: Heat, dehydration, and tight clothing increase susceptibility, while public restrooms pose no higher threat than private ones.
- Prevention focus: Public health authorities emphasize hydration, wiping front-to-back, and avoiding irritants like bubble baths.
Why the Misconception Persists—and Why It’s Harmful
For decades, the idea that cystitis spreads via toilet seats has persisted in pop culture, reinforced by outdated hygiene advice. A 2023 review of 12 studies published in the Journal of Infectious Diseases found zero evidence linking toilet-seat contact to urinary tract infections. Yet the myth continues to influence behavior, particularly among women, who already face higher infection rates due to shorter urethras.
“People avoid public restrooms because of this fear, which can lead to dehydration and worsen symptoms,” said Dr. Elena Vasquez, a urogynecologist at the European Society for Sexual Medicine. “The real culprits are bacteria from the perineal area entering the urethra—not germs on a toilet seat.”
Public health officials in France, where the guidance originated, note that 90% of cystitis cases are caused by Escherichia coli bacteria from the digestive tract. These bacteria reach the urethra through improper wiping, sexual activity, or holding urine for extended periods—none of which involve toilet seats.
What Actually Increases Your Risk—And How to Reduce It
The summer months heighten cystitis risk due to three key factors, according to the World Health Organization’s global hygiene guidelines:
- Dehydration: Hot weather increases fluid loss, concentrating urine and making it easier for bacteria to adhere to the bladder wall.
- Tight clothing: Synthetic fabrics trap moisture and heat, creating an ideal environment for bacterial growth near the urethra.
- Public restroom habits: Touching unclean surfaces (like door handles or sinks) before wiping can transfer bacteria to the perineal area.
To counter these risks, health authorities recommend:

- Drinking at least 2 liters of water daily, more if exercising or in hot climates.
- Wiping from front to back after using the toilet to prevent fecal bacteria from entering the urethra.
- Avoiding bubble baths, scented soaps, and douches, which disrupt the natural pH balance of the urinary tract.
- Urinating before and after sexual activity to flush out potential bacteria.
- Choosing loose, breathable fabrics (like cotton) over synthetic materials during warm weather.
Debunking the Toilet Seat Myth: What the Science Says
The toilet seat myth gained traction in the 1970s, when germ theory was less understood. Modern studies, however, have debunked it:
- A 2018 study in BMC Infectious Diseases swabbed 1,000 public toilet seats and found E. coli in only 3% of cases, none of which correlated with UTI outbreaks.
- A 2021 meta-analysis in Clinical Microbiology Reviews concluded that cystitis is not contagious and cannot be transmitted through surfaces.
- Public health records show no spikes in UTI cases after high-profile outbreaks of other infections (like norovirus) linked to contaminated surfaces.
“The idea that a toilet seat is a vector for cystitis is like blaming a doorknob for the flu,” said Dr. Mark Reynolds, a microbiologist at the Canadian Public Health Agency. “The bacteria causing UTIs live in our own bodies. The risk comes from how we interact with them, not from sitting on a seat.”
Summer-Specific Risks: Heat, Travel, and Behavior
Travelers and outdoor workers face elevated cystitis risks this season due to:
- Limited restroom access: Holding urine for long periods increases bladder pressure and bacterial adherence.
- Poor hydration habits: Many people reduce water intake to avoid frequent bathroom stops, unaware that dehydration worsens UTI symptoms.
- Shared spaces: Public pools, gyms, and locker rooms harbor bacteria like Pseudomonas, which can cause UTIs if they enter the urethra.
For those prone to recurrent infections, urologists recommend carrying probiotics (like Lactobacillus strains) or D-mannose supplements, which may help prevent bacterial adhesion. However, these should be discussed with a healthcare provider first.
What Officials Recommend for Public Restroom Use

While toilet seats pose no risk, public restrooms still require caution to avoid other infections. Health authorities advise:
- Using paper towels or foot pedals to avoid touching faucets or door handles.
- Carrying hand sanitizer and using it after washing hands.
- Avoiding shared towels or cloths in gyms or pools.
- Disinfecting personal items (like swimsuits or workout gear) regularly.
“The focus should be on personal hygiene, not fear of public spaces,” said Dr. Vasquez. “Cystitis is manageable when you understand the real risks—and the toilet seat isn’t one of them.”
What’s Next: Research and Policy Shifts
Public health campaigns in Europe and North America are increasingly targeting misinformation about UTI transmission, with plans to:
- Update school and workplace hygiene education to reflect current science.
- Launch digital tools to help people track UTI risk factors (like hydration and clothing choices).
- Collaborate with travel agencies to include UTI prevention tips in summer safety guides.
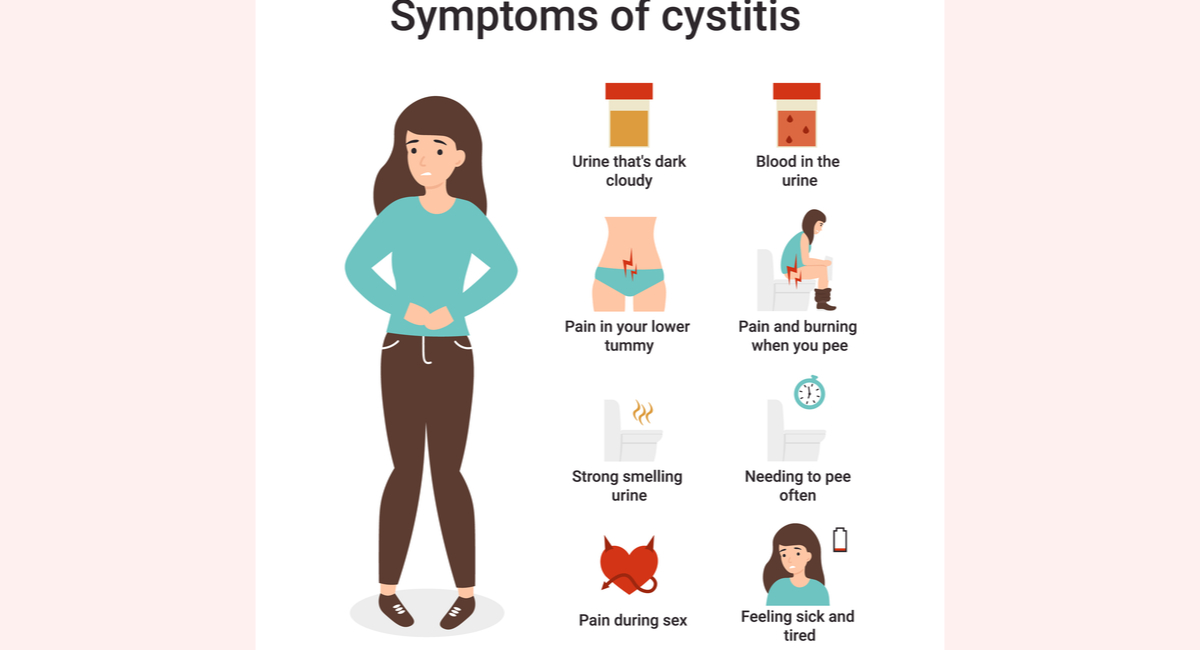
In the meantime, experts emphasize that cystitis remains highly treatable with antibiotics when symptoms (like frequent urination, pain, or cloudy urine) appear. Those with recurrent infections should seek evaluation for underlying conditions like structural abnormalities or immune deficiencies.